Evidence conflicts on iron’s role in Parkinson’s disease
Researchers debate whether too much or too little of heavy metal in the brain raises risk
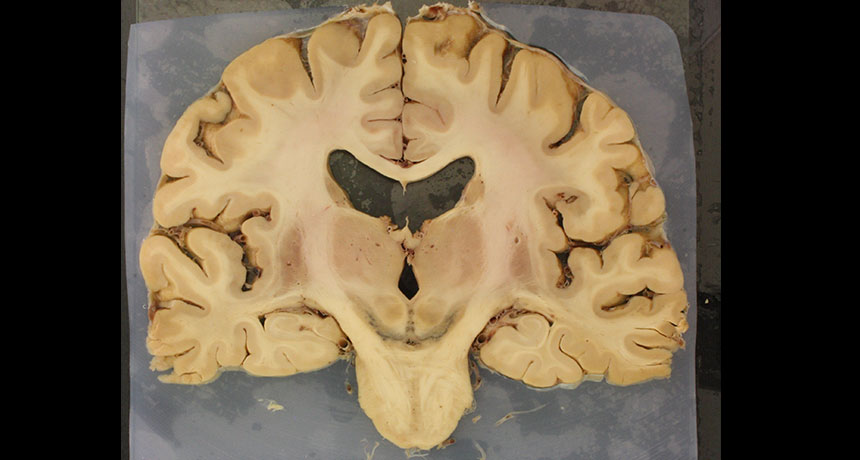
RISK FACTOR Pigmented nerve cells (black U-shape, center) in the human brain die in Parkinson’s disease, destruction that may be affected by iron levels.
Iron, says aging expert Naftali Raz, is like the Force. It can be good or bad, depending on the context. When that context is the human brain, though, scientists wrangle over whether iron is a dark force for evil or a bright source of support.
Some iron is absolutely essential for the brain. On that, scientists agree. But recent studies suggest to some researchers that too much iron, and the chemical reactions that ensue, can be dangerous or deadly, especially to nerve cells in the vulnerable brain area that deteriorates with Parkinson’s disease. Yet other work raises the possibility that those cells die because of lack of iron, rather than too much.
“There are a lot of surprises in this field,” says iron biologist Nancy Andrews of Duke University.
The idea that too much iron is dangerous captivates many researchers, including analytical neurochemist Dominic Hare of the University of Technology Sydney. “All of life is a chemical reaction,” he says, “so the start of disease is a chemical reaction as well.”
And as Raz points out, reactions involving iron are both life-sustaining and dangerous. “Iron is absolutely necessary for conducting the very fundamental business in every cell,” says Raz, of Wayne State University in Detroit. It helps produce energy-storing ATP molecules. And that’s a dirty job, throwing off dangerous free radicals that can cause cellular mayhem as energy is made.
But those free radicals are not the most worrisome aspect of iron, Hare believes. “The reaction that is much more dangerous is the reaction you get when iron and dopamine come together,” he says.
Writing in the April Brain, Hare and collaborator Kay Double of the University of Sydney argue that the chemical messenger dopamine teams up with iron to form a “toxic couple” that destroys nerve cells, or neurons. This troublesome duo, with their resulting chemical products, is particularly dangerous in the substantia nigra, the dopamine-rich part of the brain damaged in Parkinson’s, Hare and Double propose.
Dopamine has a number of breakdown products, and one of these, produced by interactions with iron, is 6-hydroxydopamine, a compound that “sounds innocuous, but it’s very damaging,” Hare says. “There are essential chemicals that you don’t want to put together.” Like gas and an open flame, dopamine and iron are best kept apart.
When protective coatings that surround and protect dopamine deteriorate, or when iron levels rise, cells can be harmed by these unintended chemical reactions. And because the substantia nigra is awash in both dopamine and iron, neurons there may be exposed to an extra-large dose of 6-hydroxydopamine.
But as evidence accumulates about the dangers of excess iron, other scientists argue that it’s a lack of iron — not too much — that endangers substantia nigra neurons.
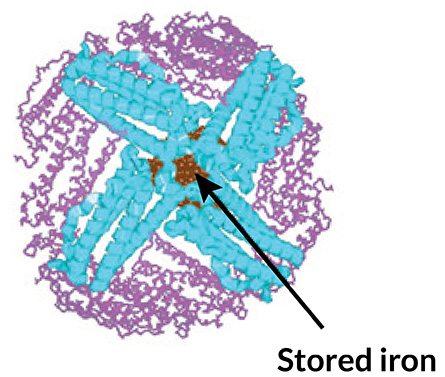
TUCKED AWAY A spherical protein called ferritin can store iron safely in an interior pocket, keeping the element from reacting with other compounds inside cells. T.A. Rouault/Nature Reviews Neuroscience 2013
This part of the brain is packed with iron, but that abundance may be deceiving, says Tracey Rouault of the National Institutes of Health in Bethesda, Md. She argues that the substantia nigra is a natural iron reservoir that simply stores the essential element for use. “People who don’t get Parkinson’s also have iron in those areas,” she says. “No one to my satisfaction has proven that the iron is excessive.”
What’s more, those elevated iron levels seen in the substantia nigra of people with Parkinson’s may not be in the neurons themselves. Instead, iron may be packed inside scavenger immune cells called microglia, cells that gobble up damaged debris. “Our eyes are fooling us,” Rouault says. Neurons that appeared to be overfed with iron may actually be starving.
Evidence of this starvation diet comes from experiments by Andrews, the Duke iron biologist, and colleagues. They genetically engineered mice to lack a protein that ferries iron into substantia nigra neurons. Without enough iron, dopamine-making neurons started to slowly wither, first losing their connections to other cells before dying. Movement problems accompanied this neural destruction, Andrews and colleagues reported March 29 in the Proceedings of the National Academy of Sciences. “If they can’t get iron in to begin with, they’re going to have a problem,” Andrews says.
Even in the midst of an environment teeming with iron, it seems that these neurons aren’t getting enough —“the opposite of what people have been saying for a long time,” Andrews says. She points to a study that found that people who gave blood frequently in a 5-year span, and as a result may have been iron-depleted, had a higher risk of Parkinson’s. Still, more work is needed to show that a functional iron deficit is behind neural damage in Parkinson’s, she acknowledges.
These iron contradictions come in part from the complexity of the brain itself. Iron can pile up in places other than in neurons, and the element exists in many forms, some of which are more reactive than others. What’s more, techniques to measure iron in a living brain don’t provide the resolution needed to see clearly what’s going on.
Meanwhile, other lines of evidence continue to suggest that too much iron is in fact hazardous. Some experiments indicate that high iron levels, which increase further with age, may damage myelin, the insulating material that protects nerve fibers, for instance. And in elderly people, high-iron, low-myelin brains were more likely to come with poorer memory performance, Tineke Steiger of the University of Lübeck in Germany and colleagues reported March 23 in the Journal of Neuroscience. Because myelin itself is iron-rich, its demise could lead to even more buildup of iron, increasing the damage, Steiger says.
T.A. Rouault/Nature Reviews Neuroscience 2013
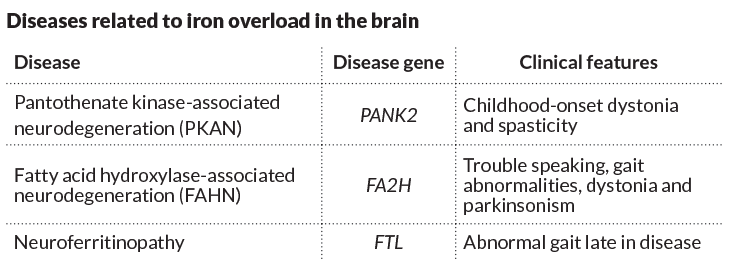
These three genetic diseases belong to a small group of disorders marked by excess iron in the brain. Rare cases like these may help clarify iron’s role in other disorders, such as Parkinson’s.
Some scientists, convinced of iron’s dangers, are pursuing a Parkinson’s therapy that strips the brain of excess iron. Their hope is that they can stop dangerous reactions by sopping up excess iron in the substantia nigra early enough to slow or prevent Parkinson’s progression.
Neurologist and neuroscientist David Devos of the University of Lille, University Hospital Center and France’s National Institute of Health and Medical Research (INSERM) is testing this approach. In a small pilot study, he and his colleagues found that an iron-slurping chelator called deferiprone may have promise. Nineteen people who took the drug — already used to treat rare diseases caused by too much iron — showed lower iron levels in their substantia nigra after six months on the drug.
More important, these people also showed slight improvements in movement, Devos and colleagues reported in 2014 in Antioxidants & Redox Signaling. The researchers have just enrolled their first two patients in what will be a much larger trial in Europe. In that trial, participants will begin the chelating treatment soon after their Parkinson’s diagnosis, a design that Devos hopes will protect vulnerable neurons before they are irrevocably damaged.
Skeptics such as Andrews don’t have confidence in this approach. “If the problem is a neuronal deficit, you could make it worse,” she says. But Hare politely disagrees. “Science is science, and people disagree a lot. We try to disprove other people’s theories,” he says. “I think the evidence there is big enough to test it.”
Editor’s note: This story was updated May 5, 2016, to correct the credit on the illustration and chart.